# Running on Teenage Collagen: Why Tendons Fail — and How We Can Help Them Heal
*By Helen How, Registered Osteopath & Sports Medicine Clinician, Helen How Clinic, Edinburgh*
Most people only think about their tendons when something goes wrong. A nagging Achilles that won’t settle. A shoulder that aches with every overhead reach. A sudden, shocking rupture in someone who felt perfectly fit the week before. And almost always, the same question follows: *why now?*
The honest answer is that “now” is rarely when the problem started. By the time a tendon hurts, the biology has usually been shifting quietly for years — sometimes decades. To understand why, and to understand why some of the treatments I use work as well as they do, it helps to know what a tendon actually is. Because it is not what most people imagine.
## A tendon is alive
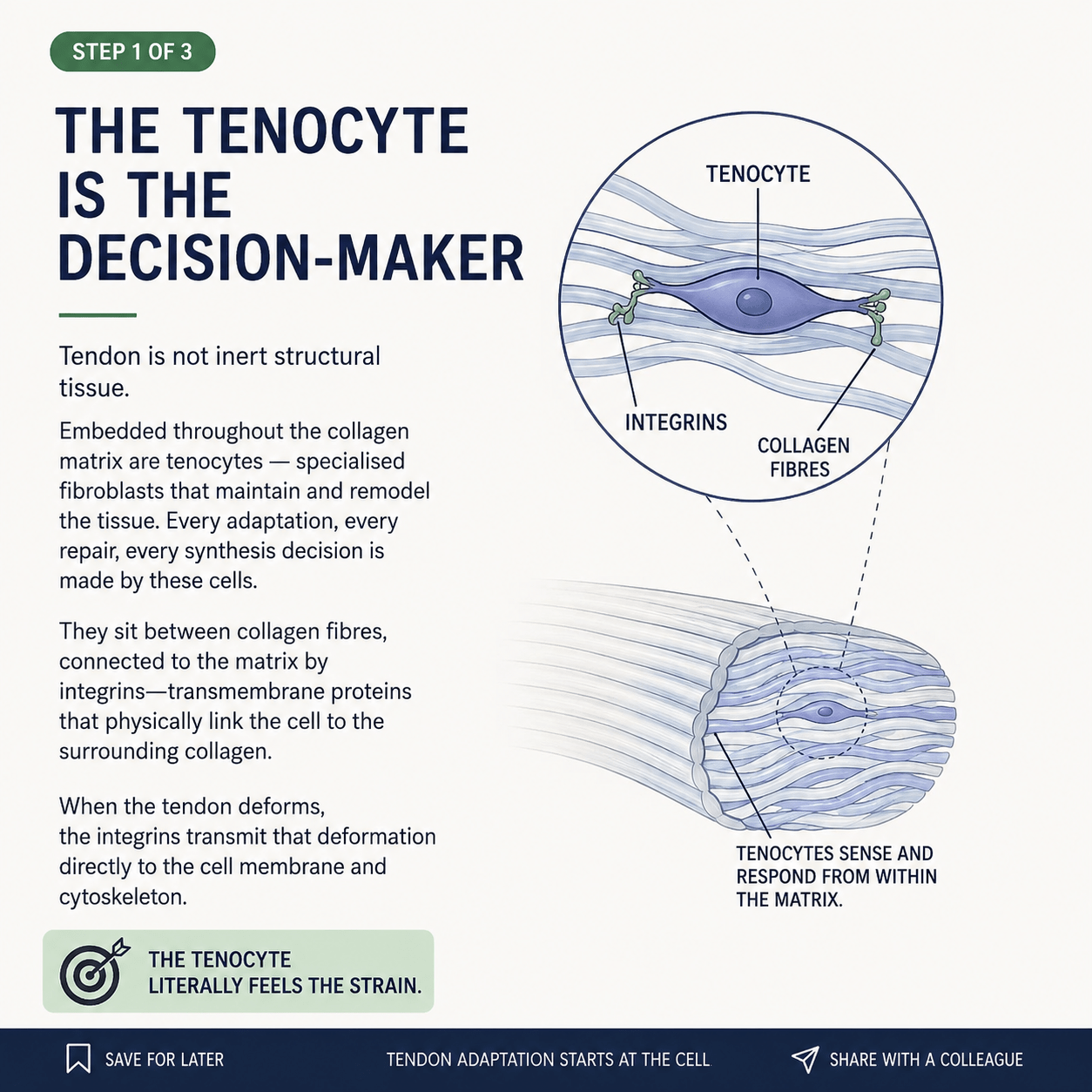
We tend to picture a tendon as a sort of inert rope — a passive cable connecting muscle to bone. It is far more interesting than that. A tendon is a living, breathing tissue, and running all the way through its dense collagen are the cells that keep it alive: the **tenocytes**.
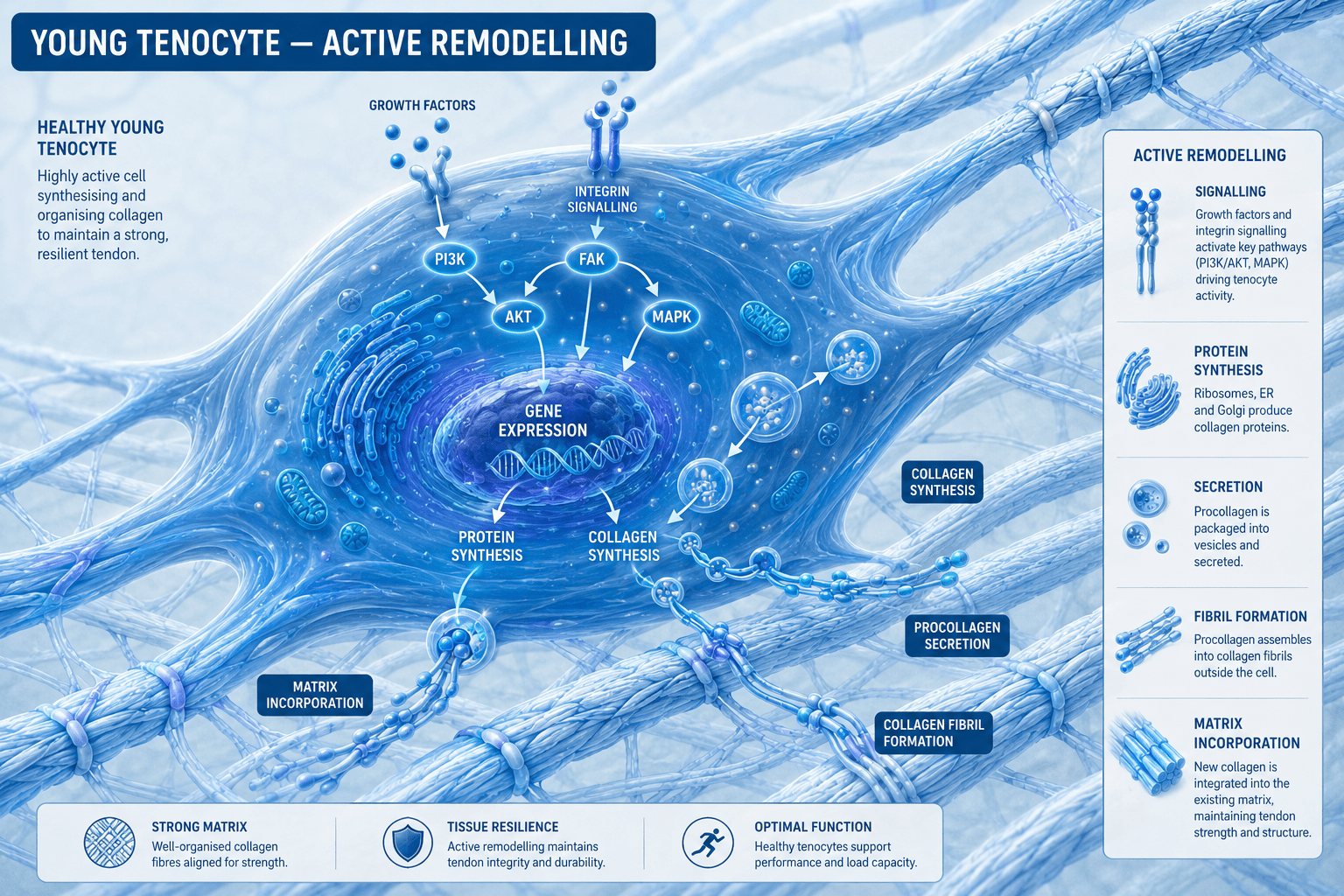
Think of tenocytes as a maintenance crew embedded throughout a great suspension bridge. They constantly sense the loads passing through the structure, and they make decisions — lay down new material here, clear away damaged material there, reinforce this section, leave that one alone. Every repair, every adaptation, every bit of strengthening a tendon ever does is carried out by these cells. A tendon is only ever as healthy as the crew maintaining it.
That maintenance is a balancing act between two opposing jobs: **building up** new collagen, and **breaking down** old or damaged collagen. In a healthy tendon these two are perfectly matched. The tissue stays strong because it is constantly, invisibly being serviced. Trouble begins — always — when breaking-down starts to outpace building-up. When that happens, the collagen slowly becomes disorganised, weaker, less able to absorb load. And here is the cruel part: this happens silently. There is no pain to warn you. Not until the tissue is already compromised.
## You are running on teenage collagen
Now for the single most surprising fact in all of tendon science — one that genuinely changes how you should think about your body.
A group of Danish researchers led by Katja Heinemeier did something ingenious. They used **carbon-14 dating** — yes, the same technique archaeologists use to date ancient bones and artefacts — to work out the age of the collagen inside living human Achilles tendons. They could do this because the nuclear bomb tests of the 1950s and 60s left a spike of radioactive carbon-14 in the atmosphere, and that spike became a kind of timestamp baked into every tissue formed during those years.
What they found was astonishing. The core, load-bearing collagen of the adult Achilles tendon carries a carbon-14 signature from the **first seventeen years of life**. After roughly the age of seventeen, that central structural collagen is barely renewed at all.
Let that sink in. The collagen doing the hard work in your tendons today was, for the most part, laid down when you were a child and a teenager. As an adult, you are not constantly rebuilding your tendons from scratch — you are *maintaining* a structure you essentially finished building at school age. You are, quite literally, running on teenage collagen.
This reframes everything. We are not stewarding a tissue that endlessly regenerates. We are looking after an irreplaceable structure that has to last a lifetime — and the only thing standing between it and gradual decline is that crew of tenocytes, doing their best to maintain what cannot easily be replaced.
## Two ways tendons fail: too much, too soon — and too old, too tired
In my clinic I see tendon trouble arrive from two completely different directions. They look like opposite problems. They end in the same place.
### The young athlete: demand outruns repair
Younger patients have a strong, responsive maintenance crew. Their tenocytes are plentiful and react well. The problem is not the cells — it’s that the **demands** they place on their tendons outpace what any tendon can keep up with.
A runner ramps up mileage too quickly. A footballer trains through a packed fixture list with no real recovery. A gym-goer chases personal bests week after week. Each session deposits a little microdamage, which is entirely normal — repair is supposed to mop it up. But remember: the core collagen barely renews, and even the surrounding matrix turns over slowly. If you keep piling load on faster than the crew can repair, damage accumulates. Breaking-down overtakes building-up. The tendon begins to degrade — quietly, painlessly — until one day it complains, or worse, tears.
These are often the fittest people you’ll meet. That’s exactly why they get caught out. They assume that because they feel strong, their tendons are keeping pace. The tissue tells a different story, and it tells it late.
### The older tendon: the crew is shrinking
In older patients the problem is the mirror image. Here it isn’t excessive demand — it’s that the **repair capacity itself has fallen**. Beautiful research reviewed by Kwan and colleagues shows three things happen to tendons as we age.
First, the crew gets smaller: tenocyte numbers fall, so there are simply fewer cells to do the maintenance. Second, the remaining cells become a little deaf: they respond more weakly to the mechanical signals that normally tell them to get to work. And third — most importantly — the threshold to wake them up rises. The very same load that would have triggered a strong rebuilding response at thirty may, at sixty-five, barely register at all.
So the older tendon faces a double bind: fewer workers, and a louder alarm needed to rouse them. Maintenance falls behind not because anyone is doing anything wrong, but because the biology has quietly moved the goalposts.
## The cells that don’t just retire — they sabotage
There is one more piece to the ageing story, and it is the part that turns a slow decline into something more active and damaging. It involves cells called **senescent cells**.
A senescent cell is one that has, in effect, retired. It has stopped dividing and stopped doing its normal job. If that were all, it wouldn’t matter much. But senescent cells don’t quietly sit in the corner. They actively secrete a toxic cocktail of inflammatory signals and matrix-destroying enzymes — a phenomenon scientists call the **SASP** (the senescence-associated secretory phenotype).
This causes three problems at once. It drives a low, grumbling inflammation through the tissue. It actively chews away at the surrounding collagen. And — remarkably — it can turn nearby healthy tenocytes senescent too, like one bad apple spoiling the barrel. So a handful of these cells can drag a whole region of tendon into decline.
A 2024 study by Stowe and colleagues showed just how damaging this is. Working with living tendon tissue, they found that when senescence took hold, collagen-building slowed right down while the collagen-destroying enzymes kept running at full tilt. The balance tipped firmly toward breakdown. They also found something that should make all of us think twice about prolonged rest: simply *unloading* a tendon — immobilising it, resting it completely — could itself trigger the senescence programme. Sometimes the instinct to “just rest it” is exactly the wrong move.
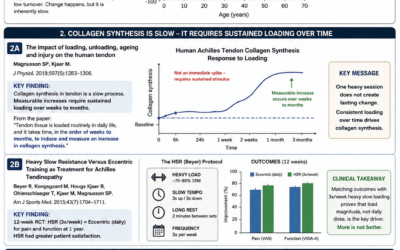
## Why loading is essential — but sometimes isn’t enough
If you’ve ever had tendon trouble, you’ll have been told to do your exercises. And rightly so. Loading a tendon — progressively, sensibly, consistently — is the single most powerful tool we have. Tenocytes respond to mechanical strain by building collagen. Loading is, and should remain, first-line treatment. None of what follows changes that.
But here is the implication of everything above. If, in an older or badly degenerated tendon, the maintenance crew has shrunk and the alarm threshold has risen, then ordinary loading may no longer be loud enough to wake the cells up. You can do your heel raises faithfully and still not generate a strong enough signal to drive real repair — not because you’re doing them wrong, but because the cells you’re trying to reach have stopped listening at that volume.
This is the gap. And it is precisely the gap that two treatments I use are designed to fill.
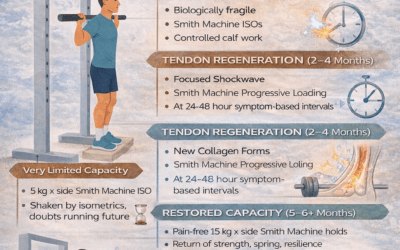
## How shockwave and EMTT help the tendon do what it can’t do alone
I have used **focused shockwave therapy** and **EMTT (Extracorporeal Magnetotransduction Therapy)** in combination since May 2019 — including right through the pandemic, when I was working as a key worker and these were among the few tools available to me. Across both the overloaded tendons of younger athletes and the worn, degenerate tendons of older patients, the results have been consistent and, in the older cases especially, often better than I’d have expected from loading alone. The science now explains why.
Both treatments do something elegant: they deliver a mechanical “wake-up” signal **directly to the tenocyte**, bypassing the raised threshold. They speak to the cell in a language it can still hear, even when ordinary loading has gone quiet.
**Shockwave** sends focused acoustic pressure waves into the tissue. In studies on human tendon cells, this has been shown to switch the cells back into action — increasing their numbers, ramping up their metabolism, and restarting the production of fresh type I and type III collagen, the very building blocks of healthy tendon (Vetrano and colleagues, 2011). It effectively re-recruits and re-energises the maintenance crew.
**EMTT** uses high-energy oscillating magnetic pulses that reach deep into the tissue, and it appears to do something rather special. A 2025 study by Mancini and colleagues, working on human tendon cells, found that EMTT switched *down* the main marker of cellular ageing (a gene called CDKN2a) while switching *up* the genes that define a healthy, productive tendon cell — and boosting collagen production along the way. In other words, EMTT seems to quieten the very senescence that drives age-related tendon decline, while turning the collagen factory back on. This is the first cellular-level clue as to why these therapies so often punch above their weight in older tendons: those are exactly the tendons carrying the heaviest burden of senescent cells.
Used together, the two complement each other. Focused shockwave provides a precise, concentrated stimulus to a specific problem area; EMTT broadens and primes the regenerative response across the whole tendon — and appears to clear away some of the senescent cells holding repair back. A randomised controlled trial in shoulder tendinopathy found the combination outperformed shockwave alone (Klüter and colleagues, 2018).
The point is not that these treatments replace good rehabilitation. They don’t. The point is that they **restore the tendon’s ability to respond** to the loading we then build on. They do, mechanically, what an overloaded or ageing tendon increasingly struggles to do for itself.
## What this means for you
If you take one thing from all of this, let it be this: tendon health is a long game, and the most important work happens long before anything hurts.
For younger, active people, the lesson is patience. Your tendons adapt far more slowly than your enthusiasm builds. Progress your training gradually, respect recovery, and don’t mistake feeling fit for being bulletproof. The collagen carrying you was laid down years ago and renews slowly — treat it accordingly.
For older people, the lesson is that decline is not inevitable surrender. Tendons remain responsive to the right stimulus at any age — the dose simply has to be smarter, and sometimes the cells need help to hear it at all. Sensible, consistent loading remains the foundation. But where a tendon has stopped responding, treatments like shockwave and EMTT can re-open the door that age has quietly been closing.
And for everyone: be wary of the instinct to simply rest a grumbling tendon into oblivion. Tendons are living tissue. They are maintained by cells that need the right kind of stimulation to stay healthy. Take that stimulation away entirely, and you may accelerate the very decline you’re trying to avoid.
Your tendons have carried you faithfully since you were a teenager. With a little understanding — and the right help when they need it — they can carry you a great deal further.
—–
*This article is written for general education and is not a substitute for individual medical advice. If you have tendon pain or an injury, please seek assessment from a qualified clinician who can advise on your specific situation.*
—–
### References & further reading
1. Heinemeier KM, Schjerling P, Heinemeier J, Magnusson SP, Kjær M (2013). *Lack of tissue renewal in human adult Achilles tendon is revealed by nuclear bomb ¹⁴C.* FASEB J 27(5):2074–2079. doi:10.1096/fj.12-225599
1. Kwan KYC, Ng KWK, Rao Y, et al. (2023). *Effect of Aging on Tendon Biology, Biomechanics and Implications for Treatment Approaches.* Int J Mol Sci 24(20):15183. doi:10.3390/ijms242015183
1. Stowe EJ, Keller MR, Connizzo BK (2024). *Cellular senescence impairs tendon extracellular matrix remodeling in response to mechanical unloading.* Aging Cell 23(11):e14278. doi:10.1111/acel.14278
1. Vetrano M, d’Alessandro F, Torrisi MR, Ferretti A, Vulpiani MC, Visco V (2011). *Extracorporeal shock wave therapy promotes cell proliferation and collagen synthesis of primary cultured human tenocytes.* Knee Surg Sports Traumatol Arthrosc 19(12):2159–2168. doi:10.1007/s00167-011-1534-9
1. Mancini M, Vetrano M, Traversa A, et al. (2025). *Electromagnetic Transduction Therapy (EMTT) Enhances Tenocyte Regenerative Potential: Evidence for Senolytic-like Effects and Matrix Remodeling.* Int J Mol Sci 26(15):7122. doi:10.3390/ijms26157122
1. Klüter T, Krath A, Stukenberg M, et al. (2018). *Electromagnetic transduction therapy and shockwave therapy in 86 patients with rotator cuff tendinopathy: a prospective randomized controlled trial.* Electromagn Biol Med 37(4):175–183.