Focused ESWT in Calcific Shoulder Tendinopathy: 25+ Years of Evidence, A Clear Clinical Position
Why the rotator cuff calcium deposit may be the single best-supported indication for focused shockwave in musculoskeletal medicine
If you have spent any time managing chronic shoulder pain — your own or a patient’s — you will know the particular frustration of calcific tendinopathy. The history is familiar. A few months of escalating pain, often worse at night. An ultrasound or X-ray showing a hydroxyapatite deposit, most commonly in the supraspinatus. Conservative care — NSAIDs, physiotherapy, perhaps a corticosteroid injection — that helps a little but does not resolve the underlying problem. And then the conversation about surgical excision, which neither patient nor clinician wants to have if there is a reasonable alternative.
There is a reasonable alternative. There has been for more than 25 years. And the evidence supporting it is now among the strongest in the entire shockwave literature.
This is a long-form discussion of that evidence — why high-energy focused extracorporeal shockwave therapy works for calcific shoulder tendinopathy, what the landmark trials actually show, how it compares to the other non-surgical option (ultrasound-guided needle barbotage), and how to translate the literature into a sensible clinical position.
The clinical problem
Calcific tendinopathy of the rotator cuff is characterised by deposits of hydroxyapatite calcium within the cuff tendons, most often the supraspinatus, less commonly the infraspinatus or subscapularis. The natural history is variable. Some deposits resolve spontaneously over months or years. But a substantial proportion of patients develop a clinical picture that does not resolve — chronic pain, sleep disturbance from being unable to lie on the affected side, restricted active elevation, and functional impairment severe enough to compromise occupational and recreational life.
First-line treatment is conservative: anti-inflammatory medication, structured physiotherapy, sometimes corticosteroid injection. For many patients this is enough. For a meaningful minority it is not. Historically the next step has been arthroscopic surgical excision, sometimes combined with subacromial decompression — an effective but invasive intervention with the usual considerations of operative risk, recovery time, and the small but real possibility of post-surgical stiffness.
Over the past quarter century, two less invasive interventions have established themselves as evidence-supported alternatives: ultrasound-guided needle barbotage (aspiration and lavage of the deposit), and extracorporeal shockwave therapy. Both work. Both have a substantial RCT literature behind them. Both deserve to be in the conversation before surgery is offered.
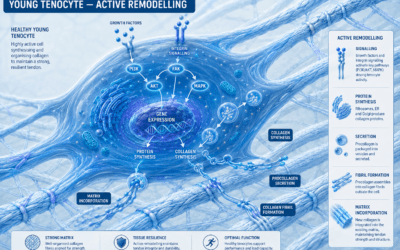
How shockwave works on a calcium deposit
The biological story is now reasonably well understood. Focused shockwave is a mechanotransductive stimulus — short-duration, high-amplitude acoustic pulses that travel through tissue and concentrate energy at a defined focal point. When that focal point is the calcium deposit, several things happen simultaneously.
Mechanically, the shockwave produces cavitation effects that fragment the calcific deposit, breaking the dense hydroxyapatite into smaller particles that can be resorbed by the body’s own clearance mechanisms. Biologically, the stimulus triggers a cascade of well-characterised responses in the surrounding tendon and bursa: upregulation of endothelial nitric oxide synthase (eNOS) and vascular endothelial growth factor (VEGF), driving neovascularisation; release of growth factors including TGF-β1 that promote collagen synthesis and tissue remodelling; suppression of pro-inflammatory cytokines (TNF-α, IL-6, IL-1β) through multiple parallel signalling pathways; and a shift in macrophage polarisation from the inflammatory M1 phenotype toward the reparative M2 phenotype.
In other words, focused shockwave does two things at once: it physically disrupts the deposit, and it activates a biological repair response in the tendon that allows the deposit to be cleared and the tissue around it to heal. This is why the clinical effect is not purely analgesic and not purely mechanical — it is both, working in parallel.
The landmark evidence
The shockwave literature in calcific shoulder tendinopathy is now 25 years deep. Five trials, in particular, deserve to be at the front of any clinician’s reading.
Loew et al, JBJS Br 1999 was the first major randomised controlled trial to establish ESWT efficacy in this indication. Eighty patients were randomised to high-energy ESWT, low-energy ESWT, or untreated control. The high-energy group showed significantly better Constant scores and radiographic deposit resolution at three months, setting the methodological template for everything that followed.
Gerdesmeyer et al, JAMA 2003 is the cornerstone reference. One hundred and forty-four patients with chronic calcific tendinitis were randomised to high-energy ESWT (0.32 mJ/mm²), low-energy ESWT (0.08 mJ/mm²), or sham — two sessions at two-week intervals. At six months, the high-energy group showed 31% complete deposit resorption and 32% partial resorption, against 13% and 14% in the low-energy group and only 6% and 14% in the sham group. Constant-Murley scores, pain reduction, and patient-reported function were all significantly superior with high-energy treatment. Published in JAMA, this is the trial that brought shockwave for calcific tendinopathy firmly into mainstream evidence-based medicine.
Wang et al, American Journal of Sports Medicine 2003 provided the critical durability evidence. Thirty-three shoulders were treated with a single high-energy ESWT session (0.55 mJ/mm², 1,000 impulses) and followed prospectively for two years. Eighty-seven percent of patients maintained sustained improvement. Fifty-seven point six percent achieved complete deposit resorption, with a further 30.3% showing partial resorption. These are not numbers that describe a transient analgesic response. They describe a durable resolution of the underlying pathology.
Albert et al, JBJS Br 2007 reinforced the dose-response message with a direct comparison of high-energy (0.45 mJ/mm²) versus low-energy (0.02 mJ/mm²) ESWT in 80 patients. The high-energy group showed significantly better Constant scores and pain reduction at three months, consistent with the Gerdesmeyer findings.
Ioppolo et al, Physical Therapy 2012 added another comparative trial at clinically deliverable settings, randomising 46 patients to higher-energy ESWT (0.20 mJ/mm²) versus lower-energy (0.10 mJ/mm²) over four weekly sessions. The higher-energy group showed significantly better pain, function, and deposit reduction at six months.
These five trials, taken together, establish the core clinical position: high-energy focused ESWT produces significant, durable improvements in pain, function, and radiographic deposit resorption in chronic calcific shoulder tendinopathy.
The systematic reviews and meta-analyses
If the individual RCTs were the building blocks, the pooled analyses that followed gave the conclusion definitive form.
Vavken et al, Sports Health 2009 pooled 14 studies of focused ESWT and demonstrated a weighted mean improvement of 2.8 points on the visual analogue scale for pain and 19.8 points on the Constant-Murley score versus control, with dose-responsive resorption of calcific deposits.
Huisstede et al, Manual Therapy 2011 reviewed evidence for both calcific and non-calcific rotator cuff tendinosis. Their conclusion was clinically important: there is moderate to strong evidence supporting ESWT for calcific tendinopathy, but only weaker evidence for non-calcific presentations. The distinction matters when setting patient expectations.
Ioppolo et al, Archives of Physical Medicine and Rehabilitation 2013 focused specifically on six-month follow-up data and confirmed that both clinical improvement and deposit resorption are sustained at half a year post-treatment.
Bannuru et al, Annals of Internal Medicine 2014 brought ESWT decisively into internal medicine guidance. Their systematic review concluded that high-energy ESWT is effective for improving both pain and shoulder function in chronic calcific shoulder tendinitis, with meaningful effects on deposit resorption.
Verstraelen et al, Clinical Orthopaedics and Related Research 2014 is, in my view, the single most useful piece of evidence on the dose question. This meta-analysis pooled high-quality RCTs comparing high-energy versus low-energy ESWT and concluded definitively that high-energy is significantly superior for both clinical outcomes and radiographic resorption.
Three convergent messages
Reading the literature as a whole, three messages emerge clearly and repeatedly.
1. High-energy beats low-energy
This is the clearest dose-response relationship anywhere in the shockwave literature. Multiple RCTs and the Verstraelen 2014 meta-analysis converge on the same finding: high-energy protocols (0.28–0.55 mJ/mm² and above) consistently outperform low-energy approaches. If a clinician is selecting ESWT for a calcific deposit, the energy density needs to be high enough to do the job. Under-dosing is a real and avoidable cause of treatment failure.
2. Focused outperforms radial at depth
Radial pressure wave therapy has a legitimate role in shoulder pain — particularly for the myofascial and superficial enthesopathic components that often accompany calcific tendinopathy. But for the calcium deposit itself, sitting at depth within the rotator cuff, focused shockwave delivers energy more reliably to the target. The physics is straightforward: focused waves converge to a defined focal point with minimal attenuation along the path; radial waves attenuate substantially with depth, delivering most of their energy at the surface and progressively less below. The two technologies are complementary, not interchangeable — and for the deposit itself, focused is the evidence-supported choice.
3. Outcomes are durable
This is not a treatment that produces a temporary analgesic effect and then loses ground. Wang’s two-year follow-up showed 87% sustained improvement and 57.6% complete deposit resorption. Daecke et al, Orthopade 2002 demonstrated maintenance of clinical benefit at four years. Lee et al, Journal of Shoulder and Elbow Surgery 2011 confirmed midterm durability across multiple studies. The pattern in the data is one of genuine pathological resolution rather than symptomatic suppression.
ESWT versus ultrasound-guided needling
The other major non-surgical option for calcific shoulder tendinopathy is ultrasound-guided needle barbotage — needle aspiration and lavage of the deposit, usually combined with a subacromial corticosteroid injection.
Louwerens et al, Arthroscopy 2020 is the most important head-to-head trial. Patients with chronic calcific rotator cuff tendinitis were randomised to ultrasound-guided needling combined with corticosteroid injection, or to high-energy focused ESWT. Both groups improved significantly. The needling group showed faster initial deposit resorption and earlier pain relief; the ESWT group caught up over time, with the two treatments showing equivalent longer-term outcomes.
The clinical implication is straightforward and worth stating clearly: these treatments are complementary, not competing. Needle barbotage is more invasive but produces faster initial results. Focused ESWT is non-invasive, requires no injection or anaesthesia, and achieves equivalent longer-term outcomes. Choice between them is a clinical decision based on patient preference, deposit characteristics (size, density, location), local expertise, and tolerance for an injection-based procedure. Neither is inherently superior. Both belong in the toolkit.
A note on non-calcific rotator cuff tendinopathy
The evidence base for ESWT in non-calcific rotator cuff tendinopathy is meaningfully weaker than for calcific disease, and patient expectations should reflect this. Kamonseki et al, American Journal of Physical Medicine and Rehabilitation 2024 systematically reviewed the non-calcific evidence and found smaller, less consistent effect sizes than in calcific presentations, though some short-term pain benefit over sham was demonstrable. Galasso et al, BMC Musculoskeletal Disorders 2012 had earlier reached a similar conclusion in a double-blind RCT in non-calcific supraspinatus tendinopathy: modest short-term benefit over placebo, smaller than the effects routinely seen with a calcium deposit to target.
ESWT works best when there is something to break up. Setting that expectation early avoids disappointment later.
A practical clinical position
Drawing all of this together into something a clinician can act on:
For a patient with chronic calcific tendinopathy of the rotator cuff who has failed first-line conservative management, high-energy focused ESWT is a strongly evidence-supported next step before surgical excision is considered. The recommended parameters from the literature are:
• Modality: focused ESWT (piezoelectric, electromagnetic, or electrohydraulic generator)
• Energy flux density: 0.28–0.55 mJ/mm² (high-energy)
• Pulses per session: 1,500–2,000
• Number of sessions: 2 typically; up to 4 in resistant cases
• Interval: 1–2 weeks between sessions
• Targeting: ultrasound-guided onto the deposit where available
• Anaesthesia: not required; the treatment is well tolerated unaided
A pragmatic decision pathway might look like this: conservative care first, with NSAIDs, structured physiotherapy, and consideration of corticosteroid injection. If pain and dysfunction persist beyond three months, discuss the two main interventional options — ultrasound-guided barbotage and high-energy focused ESWT — and let the patient choose between them on the basis of their preferences and the practicalities of access. Surgery becomes a consideration only if both non-surgical interventions have failed.
The bigger picture
Calcific shoulder tendinopathy is one of the cleanest, most consistent indications in all of musculoskeletal medicine for focused extracorporeal shockwave therapy. The evidence is now a quarter of a century deep, has been pooled in multiple high-quality meta-analyses, and consistently points in the same direction: high-energy focused ESWT works, the effects are durable, and it offers patients a genuine alternative to surgery.
The infographic accompanying this post summarises the key data points at a glance. For colleagues who want to dig deeper, I have compiled a full clinician reference PDF with the landmark trials, systematic reviews, comparative studies, and parameter recommendations linked through to their DOIs.
If your shoulder patient has a calcium deposit and has failed conservative care, the conversation about next steps should include high-energy focused ESWT. The evidence has been there for a long time. It is worth using.
Key references
Gerdesmeyer L, et al. Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial. JAMA 2003;290:2573–2580.
Loew M, et al. Shock-wave therapy is effective for chronic calcifying tendinitis of the shoulder. JBJS Br 1999;81:863–867.
Wang CJ, et al. Shock wave therapy for calcific tendinitis of the shoulder: a prospective clinical study with two-year follow-up. Am J Sports Med 2003;31:425–430.
Albert JD, et al. High-energy extracorporeal shock-wave therapy for calcifying tendinitis of the rotator cuff: a randomised trial. JBJS Br 2007;89:335–341.
Ioppolo F, et al. Extracorporeal shock-wave therapy for supraspinatus calcifying tendinitis: a randomized clinical trial comparing two different energy levels. Phys Ther 2012;92:1376–1385.
Bannuru RR, et al. High-energy extracorporeal shock-wave therapy for treating chronic calcific tendinitis of the shoulder: a systematic review. Ann Intern Med 2014;160:542–549.
Verstraelen FU, et al. High-energy versus low-energy extracorporeal shock wave therapy for calcifying tendinitis of the shoulder: which is superior? A meta-analysis. Clin Orthop Relat Res 2014;472:2816–2825.
Vavken P, et al. Focused extracorporeal shock wave therapy in calcifying tendinitis of the shoulder: a meta-analysis. Sports Health 2009;1:137–144.
Ioppolo F, et al. Clinical improvement and resorption of calcifications in calcific tendinitis of the shoulder after shock wave therapy at 6 months’ follow-up. Arch Phys Med Rehabil 2013;94:1699–1706.
Huisstede BM, et al. Evidence for effectiveness of extracorporeal shock-wave therapy (ESWT) to treat calcific and non-calcific rotator cuff tendinosis — a systematic review. Man Ther 2011;16:419–433.
Lee SY, et al. The midterm effectiveness of extracorporeal shockwave therapy in the management of chronic calcific shoulder tendinitis. J Shoulder Elbow Surg 2011;20:845–854.
Louwerens JKG, et al. Comparing ultrasound-guided needling combined with a subacromial corticosteroid injection versus high-energy extracorporeal shockwave therapy for calcific tendinitis of the rotator cuff: a randomized controlled trial. Arthroscopy 2020;36:1823–1833.
Kamonseki DH, et al. Extracorporeal shockwave therapy for the treatment of noncalcific rotator cuff tendinopathy: a systematic review and meta-analysis. Am J Phys Med Rehabil 2024;103:471–479.
Galasso O, et al. Short-term outcomes of extracorporeal shock wave therapy for the treatment of chronic non-calcific tendinopathy of the supraspinatus: a double-blind, randomized, placebo-controlled trial. BMC Musculoskelet Disord 2012;13:86.
Helen How Clinic, 14 Craighall Gardens, Edinburgh EH6 4RJ. Equipment: Storz Medical DUOLITH SD1 (focused ESWT), MASTERPULS (radial), MAGNETOLITH (