The Achilles Tendon Rupture Rate Is Rising. Why Is Nobody Talking About It?
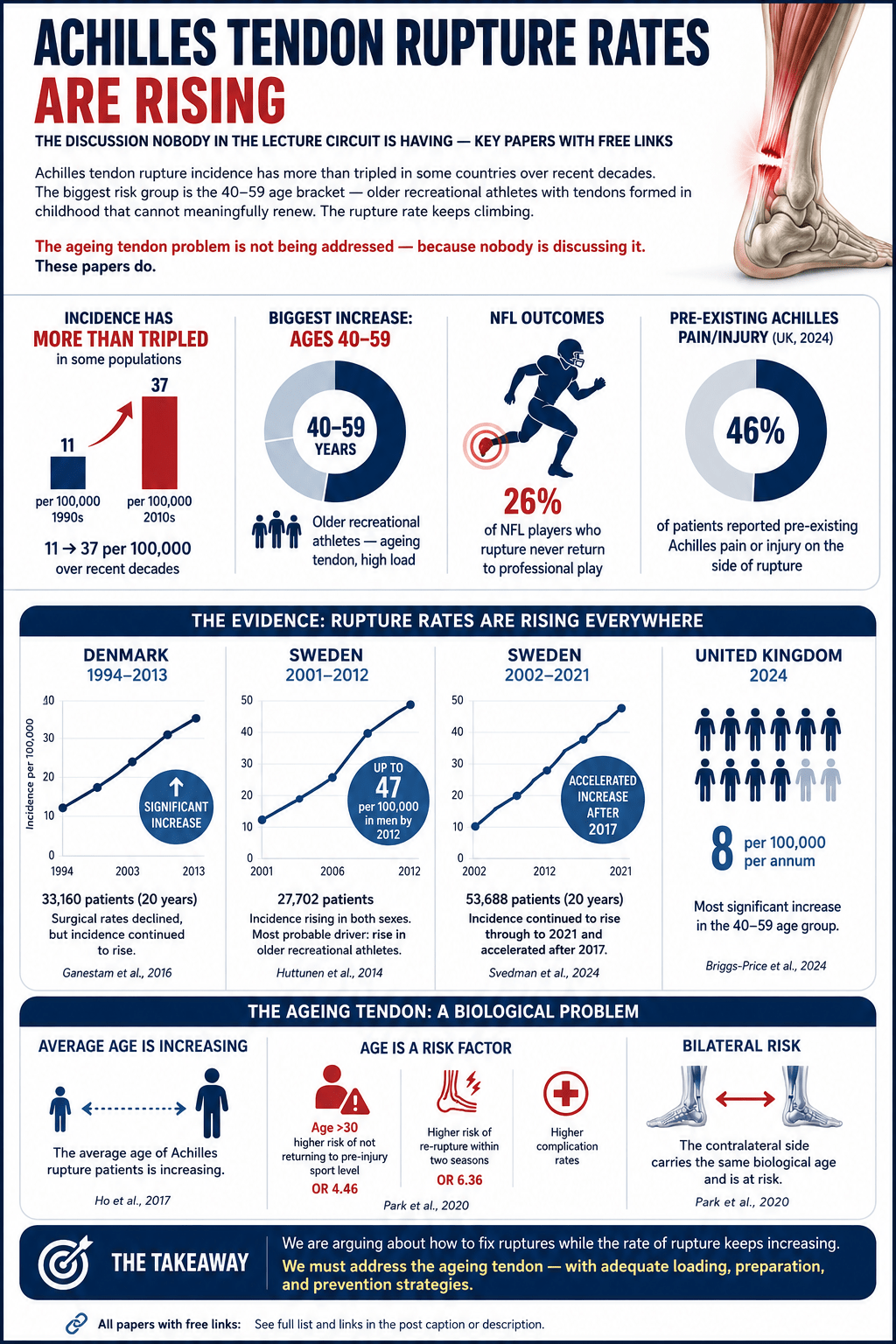
Achilles tendon rupture incidence has more than tripled in some populations over the last few decades. Not doubled. Tripled. From 11 to 37 per 100,000 in some countries. The biggest growth group is not young elite athletes. It is the 40-59 age bracket — older recreational athletes who believe they are fit, active and healthy, and whose tendons are simply not prepared for the loads being placed on them.
The conference circuit keeps running courses on eccentric protocols, surgical techniques and return-to-sport timelines. The rupture rate keeps climbing anyway.
The Numbers
A Danish nationwide registry study of 33,160 patients over 20 years found a statistically significant increase in rupture incidence across the entire period (Ganestam et al., 2016). Sweden reported 27,702 ruptures between 2001 and 2012, with incidence rising in both men and women — up to 47 per 100,000 per year in men by 2012 (Huttunen et al., 2014). A more recent Swedish study extended the data to 53,688 ruptures between 2002 and 2021 and found the increase not only continued but accelerated after 2017 (Svedman et al., 2024). Globally, a bibliometric analysis of over 3,500 studies found incidence had risen from 11 to 37 per 100,000 — more than tripled — over recent decades (Wang et al., 2023).
A 2024 UK emergency department study added a finding that should stop every clinician in their tracks: 46% of patients who ruptured their Achilles tendon reported pre-existing Achilles pain or injury on the same side before it failed completely (Briggs-Price et al., 2024). Nearly half had a symptomatic tendon that was never adequately loaded or rehabilitated. It did not rupture out of nowhere. It was already compromised.
The Aaron Rodgers Moment
In September 2023, Aaron Rodgers — the newly acquired $75 million quarterback for the New York Jets — ruptured his Achilles tendon four snaps into his first game on national television. The reaction was disbelief. It should not have been surprising.
Timothy Hewett and colleagues published a clinical insight paper in the International Journal of Sports Physical Therapy asking the question directly: have Achilles tendon injury rates in the NFL risen to unacceptably high levels, and if so, why? (Hewett et al., 2024). Their answer pointed to increasing player size and BMI, fixture and schedule demands, and — critically — the absence of sufficient preparatory tendon loading. Heavy slow resistance training. The thing that is free, evidence-based, and consistently underutilised.
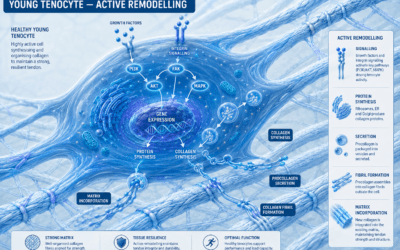
The Biology Nobody Is Discussing
Here is what the lecture circuit is not adequately addressing.
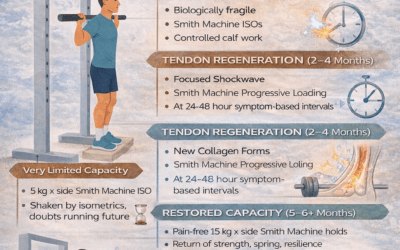
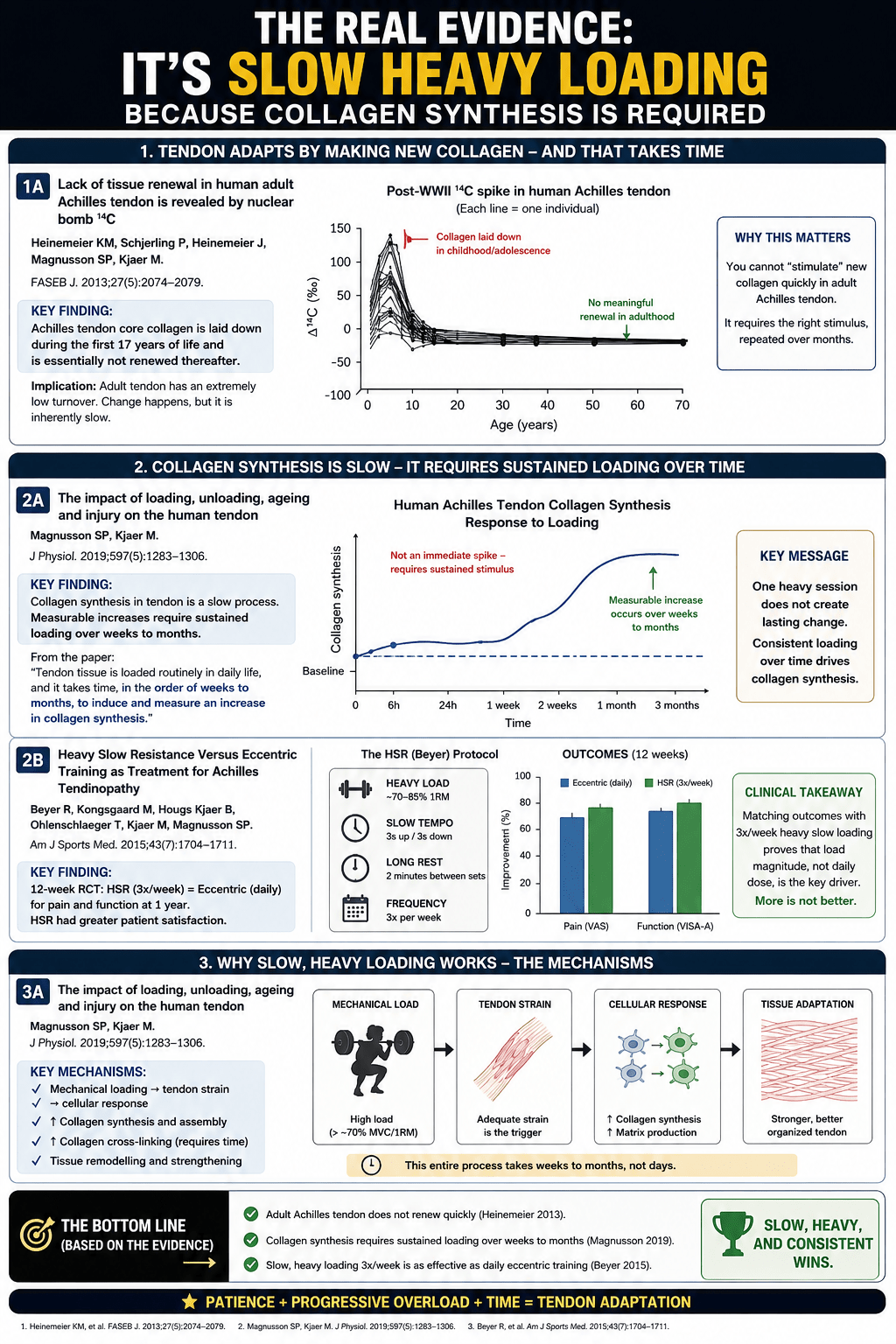
In 2013, Heinemeier and colleagues used post-World War II nuclear test carbon-14 — the so-called bomb pulse — to measure lifelong tissue turnover in human Achilles tendons. What they found was stark: Achilles tendon core collagen is laid down during the first 17 years of life and is essentially not renewed thereafter (Heinemeier et al., 2013). The tendon a 50-year-old is running on was formed when they were a teenager. It cannot regenerate passively. It cannot be stimulated to renew quickly. Change happens, but it is inherently slow.
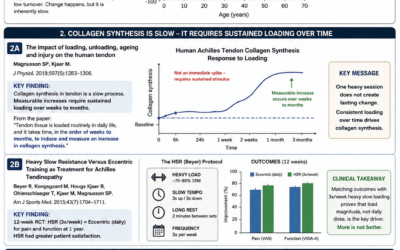
Magnusson and Kjaer’s 2019 review of loading, unloading, ageing and injury in human tendon confirmed that measurable increases in collagen synthesis require sustained loading over weeks to months — not days (Magnusson & Kjaer, 2019). One heavy session does not create lasting structural change. Consistent loading over time does.
The ageing active population — the weekend warrior in their 40s and 50s — is being asked to perform at high recreational loads with tendons that were formed decades ago, that cannot renew rapidly, and that have in many cases never been systematically loaded with sufficient magnitude and tempo to build meaningful capacity.
What The Evidence Actually Supports
Beyer and colleagues published a randomised controlled trial in 2015 directly comparing traditional daily eccentric heel drops against heavy slow resistance training three times per week (Beyer et al., 2015). Both groups improved equally in pain and function at one year. Heavy slow resistance showed greater patient satisfaction at 12 weeks. Three sessions per week matched daily eccentric training. Load magnitude — not daily dose — is the key variable.
Arampatzis and colleagues established that tendons must be loaded above approximately 70% of maximum voluntary contraction to produce meaningful structural change (Arampatzis et al., 2007, 2010). Body weight exercises alone are insufficient for most patients. Slow tempo — three to four seconds up, three to four seconds down — allows the tendon time to deform viscoelastically, generating the fibril-level mechanical signal that tenocytes actually respond to. Fast repetitions do not.
Kongsgaard and colleagues demonstrated that heavy slow resistance training changed fibril morphology and cross-link composition in tendinopathic tendons — structural change, not just symptom relief (Kongsgaard et al., 2009). Corticosteroid injection produced short-term pain relief and worse outcomes at six months.
The Translation Problem
More papers on Achilles tendon injury were published in 2021 than in any previous year. Publications increased fivefold between 2000 and 2021. The evidence base is not the problem. The translation is.
The rupture rate is rising because an ageing active population with irreplaceable tendons is not being systematically prepared for the loads they are placing on them. The biology has been understood since 2013. The loading evidence has been clear since 2015. The clinical framework exists.
Slow. Heavy. Twice or three times a week. Weeks to months of consistent loading. Patience as a clinical prescription.
The rate goes up anyway. Something is not getting through.
References
Beyer R et al. Am J Sports Med. 2015;43(7):1704–1711. https://pubmed.ncbi.nlm.nih.gov/26018970/
Briggs-Price et al. PLOS ONE. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11192343/
Ganestam A et al. Knee Surg Sports Traumatol Arthrosc. 2016;24(12):3730–3737. https://pubmed.ncbi.nlm.nih.gov/25697284/
Heinemeier KM et al. FASEB J. 2013;27(5):2074–2079. https://pmc.ncbi.nlm.nih.gov/articles/PMC3633810/
Hewett TE et al. Int J Sports Phys Ther. 2024;19(2):145–147. https://pubmed.ncbi.nlm.nih.gov/38313673/
Huttunen TT et al. Am J Sports Med. 2014;42(10):2419–2423. https://pubmed.ncbi.nlm.nih.gov/25056989/
Kongsgaard M et al. Scand J Med Sci Sports. 2009;19(6):790–802. https://pubmed.ncbi.nlm.nih.gov/19793213/
Magnusson SP & Kjaer M. J Physiol. 2019;597(5):1283–1298. https://pmc.ncbi.nlm.nih.gov/articles/PMC6395417/
Svedman S et al. Br J Sports Med. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11261689/
Wang C et al. Front Surg. 2023. https://www.frontiersin.org/articles/10.3389/fsurg.2023.1051429/full