A real Achilles case — and why the timeline matters
This runner came to me on the recommendation of another committed runner who’d responded well to focused shockwave. He arrived with severe, painful mid-portion Achilles tendinopathy and a history of multiple rehab attempts, none of which had worked. By the time I saw him he’d quietly concluded his running career might be over — and for him that wasn’t a small thing. Running isn’t just something he does; he loves it.
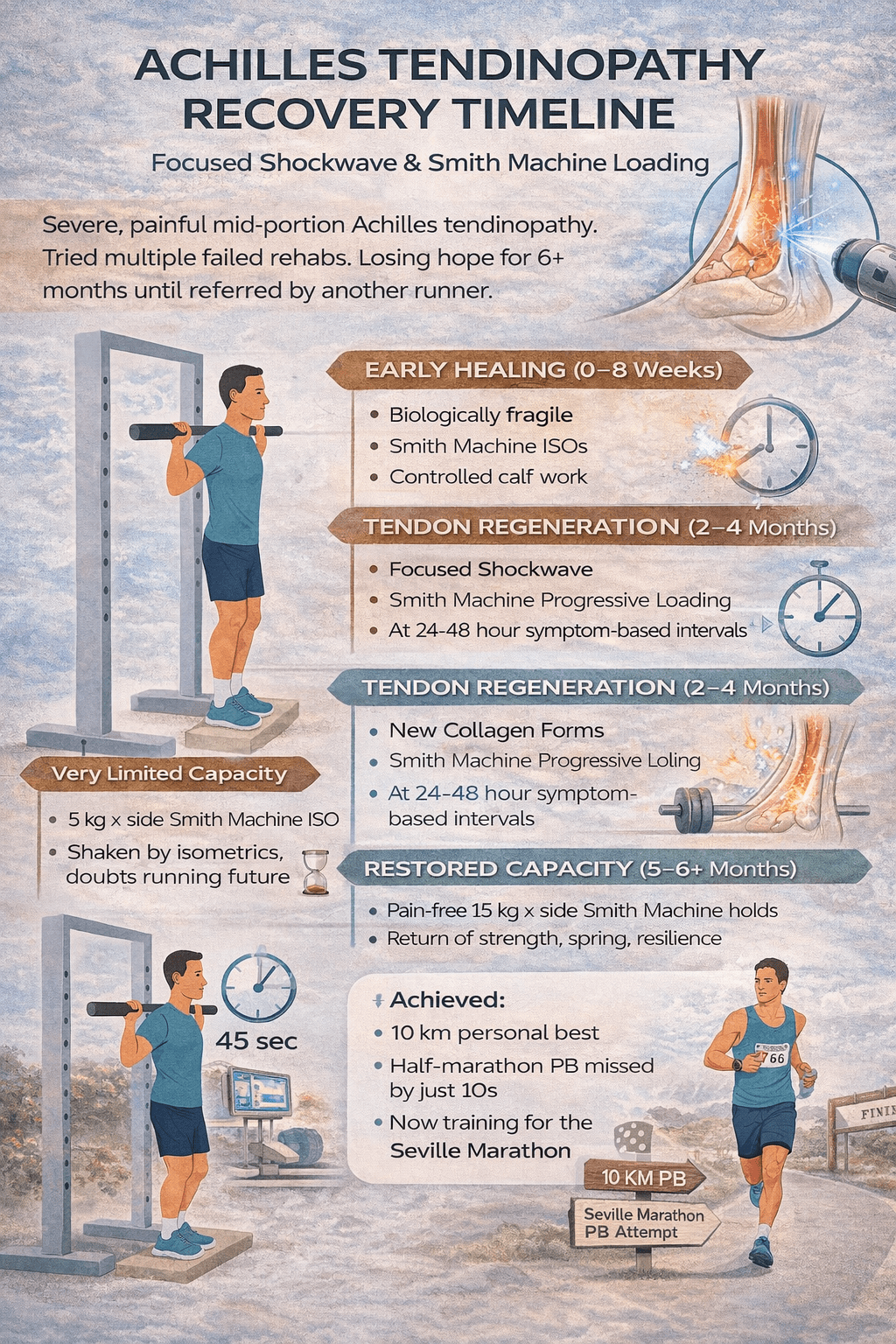
He’s 38, a new dad to a young baby, fitting training in wherever he can. Stopping completely was never realistic. What he needed wasn’t *more* rehab — it was the *right* rehab, applied over the right biological timeframe.
The plan
We kept it deliberately simple and worked with the tendon’s biology rather than against it:
– Focused shockwave therapy, appropriately spaced, as an adjunct
– Early Smith machine isometrics to load the tendon safely while it was painful
– Gradual progression to heavier, controlled Smith machine loading
– Running guided by next-day symptoms rather than fear
Early on his capacity was very limited — on the Smith machine he could manage only about 5 kg per side, and sustained holds were a struggle. Over the following months that progressed to 15 kg per side, held with control and tolerance.
Why the timeline does the heavy lifting
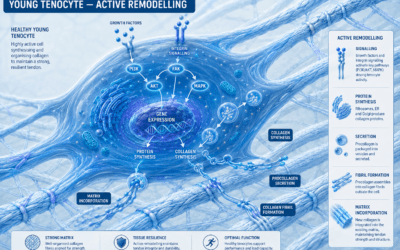
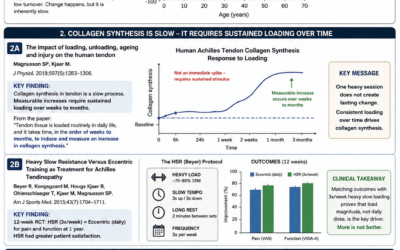
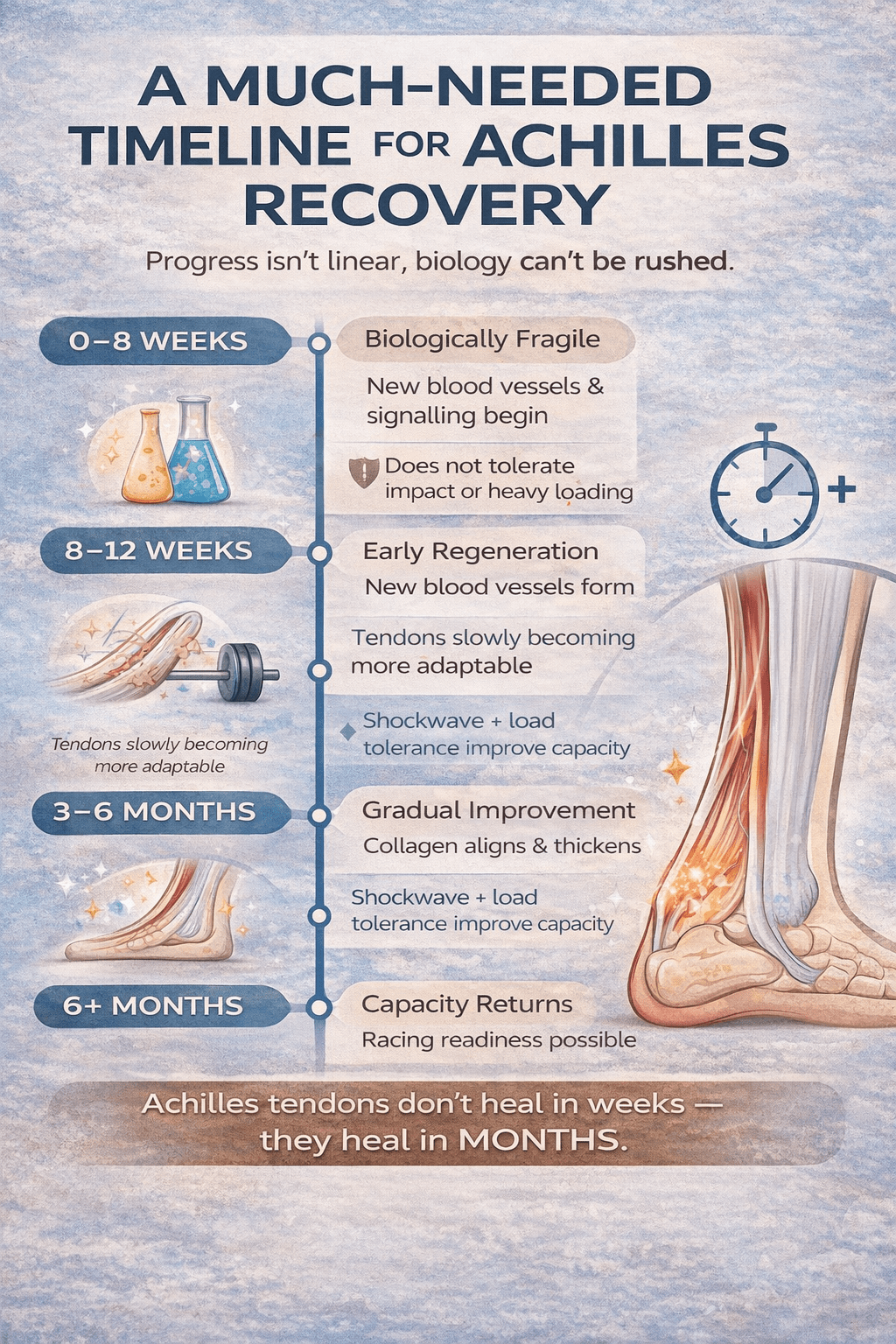
Tendon doesn’t reorganise on a weekly schedule. Magnusson and Kjaer’s 2019 review in *The Journal of Physiology* lays out the basic picture: loading raises the tendon’s cellular and molecular activity and, over time, its stiffness, while inactivity does the reverse. But the meaningful structural change is slow. Their work also shows just how slow tendon adaptation is after injury — after an Achilles rupture repair, for instance, metabolic activity and stiffness keep changing for 6 to 12 months. The 2012–2025 rehab literature echoes this for tendinopathy specifically: meaningful recovery typically takes three to six months of consistent loading, not weeks.
The encouraging part is that loading genuinely changes the tissue, not just the symptoms. In patellar tendinopathy, heavy slow resistance training has been shown to shift collagen fibril morphology back toward normal and to alter the tendon’s cross-link composition (Kongsgaard and colleagues). That’s the kind of change you can’t rush — and it’s why patience, not intensity, is usually what’s been missing in failed rehabs.
Why heavy, slow loading — not just “eccentrics”
A lot of runners arrive convinced they need to be doing eccentric heel drops. The evidence doesn’t really support treating the eccentric phase as magic. As Couppé and colleagues argued in their 2015 clinical commentary, the tendon is a passive structure: for a given load and range, it sees the same stretch whether the muscle is lengthening or shortening, and there’s no convincing clinical evidence that isolated eccentric loading beats other loading approaches. What the tendon responds to is the magnitude and duration of load.
That’s exactly why the Smith machine suited this case. It let me deliver heavy, controlled, slow loading with precise progression — and a heavy slow resistance approach has been shown to match daily eccentric protocols for Achilles tendinopathy (Beyer and colleagues) while being far less time-hungry. For a new dad with almost no spare time, three focused sessions a week beat a daily heel-drop marathon he’d never sustain. Adherence is part of the prescription.
Why we spaced the loading
Heavy loading every single day isn’t better — it’s often worse. The anabolic response to a bout of loading lasts a couple of days, and the literature is honest that studies directly testing recovery timing are limited; but in practice, daily heavy loading without rest tends to under-perform programmes that build in recovery. So we left room between heavy sessions and let his next-day symptoms set the pace, using a pain-monitoring approach: some discomfort during and after is acceptable, as long as it isn’t worse the following day.
Where shockwave actually fits
I want to be straight about this, because it’s easy to oversell. The loading is what rebuilt his capacity. Across the tendinopathy literature, progressive mechanical loading is the consistent driver of improvement, and adjuncts like shockwave sit alongside it as support, not as the active ingredient. Focused shockwave can help create a more tolerable window in which a stubborn, painful tendon will accept load — but it doesn’t replace the months of loading, and the evidence for it in mid-portion Achilles tendinopathy is moderate rather than emphatic. In this case it was a useful adjunct to the real work, not a shortcut around it.
The outcome
Once capacity returned, performance followed. He ran a 10 km personal best, came within ten seconds of his half-marathon PB, and is now training for the Seville Marathon with another PB in mind. The Achilles feels strong and responsive, even with speed work back in the programme.
What this case reinforces
– Tendons heal on a timeline of months, not weeks
– Load — heavy, slow, progressive — is what builds lasting capacity; the “eccentric vs concentric” debate matters far less than the load itself
– Recovery between heavy sessions is part of the programme, not a break from it
– Shockwave is a helpful adjunct, not the thing that does the healing
– A plan the patient can actually sustain beats a “perfect” plan they’ll abandon
This was never about proving a point. It was about giving someone their running back.
*Shared with full patient consent. This describes one person’s response and isn’t a guaranteed outcome; every tendon and every runner is different.*