What the Japanese Learnt About Racehorse Tendons — and What the Korean Evidence Confirms in Humans
A clinical commentary on the under-dosing of human Achilles tendinopathy, and what the veterinary world has known for two decades.
The Tendon That Tells The Story
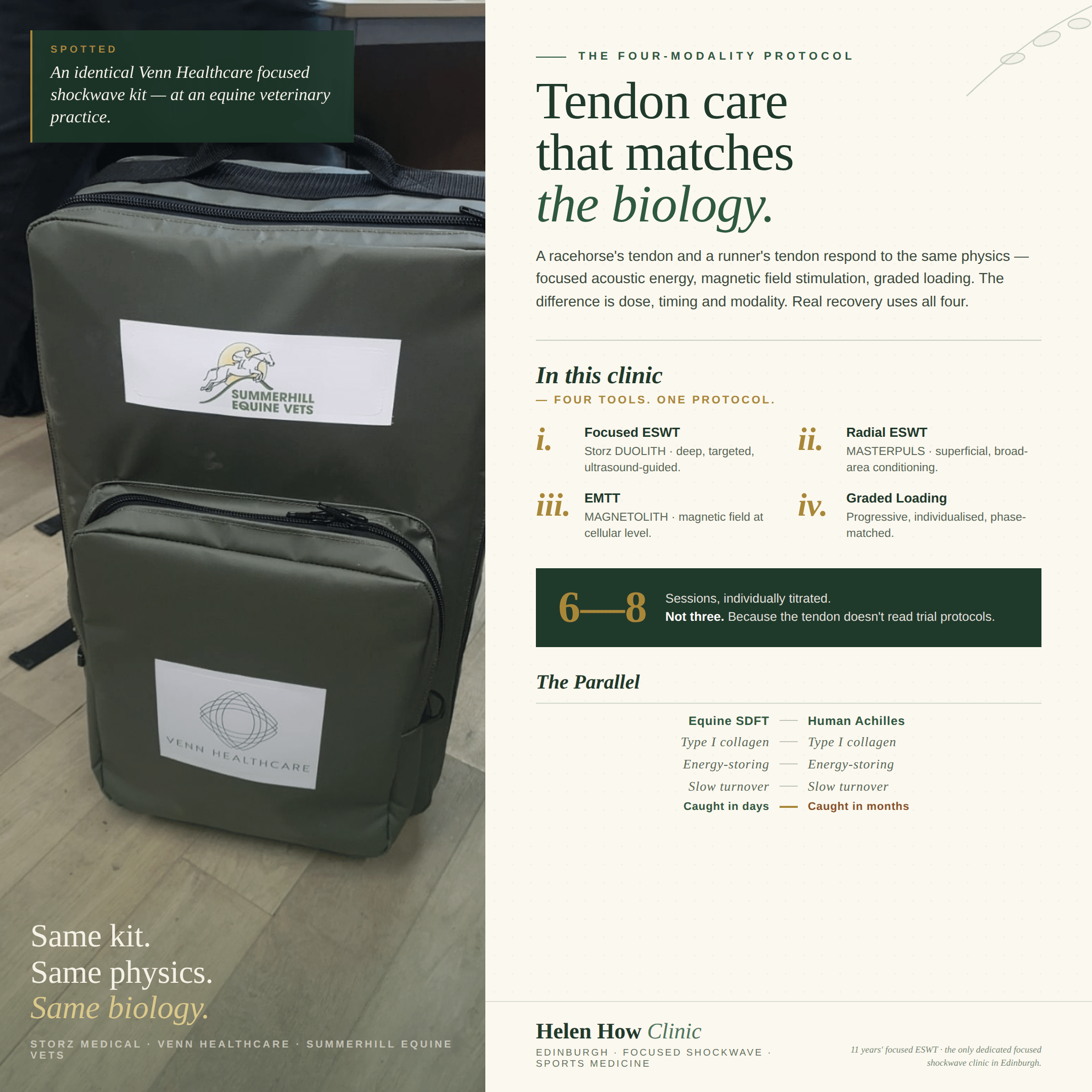
The superficial digital flexor tendon in a racehorse is biologically and functionally almost identical to the human Achilles tendon. Both are made of Type I collagen. Both are energy-storing structures, designed to absorb load and release it elastically with each stride. Both have a famously slow turnover. Both have limited capacity for true regeneration once damaged — they tend to heal with disorganised scar tissue rather than restored fibrillar architecture.
Vets even refer to the equine SDFT as “the racehorse Achilles.” The parallel is not poetic. It is anatomical, biochemical, and functional.
So a reasonable person might assume that a sport horse with a sore tendon and a runner with a sore Achilles would be assessed and treated using broadly similar principles. They are not. And the gap between the two approaches has become increasingly difficult to defend.
The Equine Model: Surveillance, Early Detection, Adequate Dose
At the Japan Racing Association’s Miho Training Centre, Thoroughbreds undergo routine ultrasound surveillance of the superficial digital flexor tendon, regardless of clinical signs. A retrospective analysis of horses scanned between 2010 and 2012 showed that an increase in tendon cross-sectional area, or the presence of subcutaneous peritendinous oedema, predicted the subsequent onset of severe tendon injury — even when there was no swelling, no heat, and no painful response on palpation.
In other words: the structural damage begins before the lameness appears. By the time clinical signs are obvious, the tendon is already in trouble. Routine imaging detects this. Clinical examination alone does not.
The Hong Kong Jockey Club cohort of 469 Thoroughbreds (Alzola et al., Equine Veterinary Journal, 2018) extended this further. Ultrasonographic parameters at presentation predicted both return to racing and re-injury risk. The implication is consistent: structural assessment changes prognosis. Waiting for symptoms is too late.
A 2025 systematic review in Frontiers in Veterinary Science quantified the equine clinical landscape. Superficial digital flexor injury accounts for approximately 46% of all limb injuries in racehorses. Of equine veterinarians surveyed, 76.8% use extracorporeal shockwave for tendon injury, and 73.6% use focused shockwave generators specifically. Treatment parameters are typically 0.15 mJ/mm² with 1,000–2,000 pulses, delivered at three-weekly intervals — note the three-week, not three-day, spacing — and repeated across multiple cycles as the lesion requires.
The equine protocol therefore has four pillars: routine surveillance, early detection, withdrawal from loading, and adequately dosed shockwave therapy delivered over an appropriate course.
Each of these four pillars is, broadly, absent from human sports medicine practice.
The Human Trial Standard: Designed for Studies, Not for Tendons
The published trial protocol for human Achilles tendinopathy has remained essentially unchanged since the early 2000s. Three weekly sessions at 0.10–0.12 mJ/mm², 2,000 shocks per session. This regimen was established by the foundational randomised controlled trials of Rompe and Furia, and has propagated through the literature largely unchallenged.
The trial regimen was never claimed to be optimal therapy. It was designed for trial logistics: a manageable number of sessions, a manageable follow-up window, a manageable energy per session that could be safely standardised across multiple centres. It is, in effect, a minimum viable dose chosen so that a randomised controlled trial could be completed.
Twenty years on, that pragmatic compromise has hardened into accepted clinical convention. The “three weekly sessions” model is what shockwave devices are programmed for, what insurance schedules reimburse, and what most clinicians deliver — even though the underlying tendon biology has not changed and the cumulative therapeutic energy delivered is, by the published authors’ own subsequent admission, often inadequate.
The Lee 2017 Reassessment: What Happens When You Dose Properly
In 2017, Lee and colleagues at Kangbuk Samsung Hospital, Seoul, published a study in the Annals of Rehabilitation Medicine that should have prompted a fundamental rethink of the human Achilles protocol. It largely did not — partly because the paper is quietly written, and partly because its conclusions are inconvenient for a field comfortable with its conventions.
Lee et al. treated 33 patients (45 feet) with chronic refractory Achilles tendinopathy who had already failed standard conservative treatment for more than six months. Their protocol was deliberately different from the trial standard:
Up to 12 weekly sessions of low-energy shockwave, at 0.10–0.11 mJ/mm² and 600 shocks per session, with treatment continued until the Roles-Maudsley Score reached “good” or “excellent.” Crucially, post-treatment soreness was used as a clinical marker of appropriate biologic dose. If soreness persisted beyond an acceptable window, the next session was deferred.
The results were striking. The immediate success rate was 71.1%. The long-term success rate, at a mean of 26 months follow-up, was 90.3%. No adverse reactions of clinical significance were reported.
These outcomes are substantially better than those reported in the original three-session trials, where success rates of 50–65% are typical. Lee et al. did not compare directly with three-session protocols in a head-to-head trial — they were not running a trial, they were treating refractory patients clinically — but the published numbers speak for themselves.
The discussion section of the paper makes the underlying point explicitly. The authors compared total effective treatment energy across protocols. Furia’s single-session high-energy approach delivered 630 mJ/mm² in one go. Rompe’s three-session protocol delivered 240 mJ/mm² per session, totalling 720 mJ/mm². Lee’s protocol delivered only 60–66 mJ/mm² per session — but cumulatively, across up to 12 sessions, reached 720–792 mJ/mm². Comparable cumulative energy. Far gentler per session. Lower risk of iatrogenic tissue damage. Better outcomes.
The conclusion writes itself: it is not the energy per session that matters most. It is the cumulative therapeutic dose, delivered in increments the tendon can tolerate without inflammatory backlash.
This is, almost exactly, the equine clinical principle.
Why the Three-Session Convention Survives
If Lee et al. published these outcomes in 2017, why has the human Achilles protocol not changed?
Three reasons, in approximate order of importance.
First, clinical inertia. Three sessions is what most physiotherapists and sports medicine clinicians are trained to deliver. Treatment device presets are configured around it. Reimbursement schedules are built around it. Changing this requires re-educating a workforce, and there is little institutional appetite for that conversation.
Second, the trial-evidence hierarchy. Clinicians are trained to follow randomised controlled trials. Lee et al. is a single-arm prospective cohort with retrospective analysis — methodologically lower in the hierarchy than an RCT, even when its outcomes are demonstrably superior. The result is that a 90.3% long-term success rate, achieved through proper dosing, is treated as weaker evidence than a 60% success rate achieved through an under-dosed RCT.
Third, denial. Many human practitioners simply do not want to hear that the equine veterinary world has been ahead of them for twenty years. The professional discomfort of being out-clinicianed by horse vets is real, and it shapes which evidence gets read and which gets quietly ignored.
Screenshot
The Clinical Implication
A tendon does not distinguish between species. It responds to three things: dose, timing, and load.
Dose means cumulative therapeutic energy at a level the tendon can biologically respond to. The trial-standard three sessions at 0.10–0.12 mJ/mm² are insufficient for most chronic Achilles cases. Six to eight sessions, individually titrated against tissue response, is closer to what the biology demands. In refractory cases, Lee et al. demonstrate that up to twelve sessions can be appropriate.
Timing means catching the lesion early — ideally before it becomes chronic — and spacing sessions to allow tissue response between treatments rather than stacking them. Three-weekly intervals, common in equine practice, allow biologic processes to unfold. Three-daily intervals do not.
Load means progressive, individualised, phase-matched graded loading throughout the treatment course. Shockwave without loading is incomplete therapy. Loading without shockwave, in chronic refractory cases, is often inadequate.
This clinic, trained by the racehorse veterinary team at Summerhill Equine Vets, applies these principles in human practice.
Closing
The Japanese learnt that tendon damage starts before lameness appears, and built surveillance accordingly. The Koreans learnt that adequate cumulative dose, gently delivered, outperforms aggressive single-session protocols. The Hong Kong cohort confirmed that ultrasonographic structural assessment changes prognosis. The 2025 Frontiers review documented that 76.8% of equine vets are already practising this way.
The human medical literature has, for two decades, been delivering an under-dosed protocol that was designed for trial convenience. The evidence to revise it is clear, peer-reviewed, freely available, and largely ignored.
A tendon does not read research papers. It responds to what is actually done to it.
References
1. Lee JY, Yoon KJ, Yi Y, et al. Long-Term Outcome and Factors Affecting Prognosis of Extracorporeal Shockwave Therapy for Chronic Refractory Achilles Tendinopathy. Annals of Rehabilitation Medicine, 2017;41(1):42–50.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5344825/
2. Tsukiyama et al. Relationship between ultrasonographic findings of suspected superficial digital flexor tendon injury and the prevalence of subsequent severe SDFT injuries in Thoroughbred horses. Japan Racing Association, Miho Training Centre.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8920721/
3. Alzola R, et al. Ultrasonographic-based predictive factors influencing successful return to racing after superficial digital flexor tendon injuries in flat racehorses: a retrospective cohort study in 469 Thoroughbred racehorses in Hong Kong. Equine Veterinary Journal, 2018;50(5):602–608.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6099230/
4. Extracorporeal shock wave therapy for equine musculoskeletal disorders: from biological mechanisms to clinical applications. Frontiers in Veterinary Science, 2025.
https://www.frontiersin.org/journals/veterinary-science/articles/10.3389/fvets.2025.1719123/full
5. Yao G, Chen J, Duan Y, Chen X. Efficacy of Extracorporeal Shock Wave Therapy for Lateral Epicondylitis: A Systematic Review and Meta-Analysis. BioMed Research International, 2020.
https://pmc.ncbi.nlm.nih.gov/articles/PMC7106907/
6. Stania M, et al. Extracorporeal Shock Wave Therapy for Achilles Tendinopathy. BioMed Research International, 2019.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6948318/
7. Rompe JD, Nafe B, Furia JP, Maffulli N. Eccentric loading, shock-wave treatment, or a wait-and-see policy for tendinopathy of the main body of tendo Achillis: a randomized controlled trial. American Journal of Sports Medicine, 2007;35:374–383.
8. Rompe JD, Furia J, Maffulli N. Eccentric loading compared with shock wave treatment for chronic insertional Achilles tendinopathy: a randomized, controlled trial. Journal of Bone and Joint Surgery (American), 2008;90:52–61.
9. Furia JP. High-energy extracorporeal shock wave therapy as a treatment for insertional Achilles tendinopathy. American Journal of Sports Medicine, 2006;34:733–740.
10. Rasmussen S, Christensen M, Mathiesen I, Simonson O. Shockwave therapy for chronic Achilles tendinopathy: a double-blind, randomized clinical trial of efficacy. Acta Orthopaedica, 2008;79:249–256.