Shoulder pain and the challenges of diagnosis of Shoulder Pain and Rotator Cuff Tears both the clinical examination differential diagnosis case history age of the patient Operate or not is challenging and complex due to ongoing research by well-known specialist shoulder specialists Dr Lennard Funk Msc, FRCS (Tr & Orth) Dr Funk latest discussion presentation considers
In this presentation will explore the literature on rotator cuff tears and the evidence for a paying cuff tears. There is great variation amongst surgeons as to the management of rotator cuff tears, biased by experience and their understanding of literature, skill levels and regional variations. I therefore undertook to try and obtain has balanced have view as possible for the reliability and relevant studies in the current literature.
Are cuff tears normal?
There is adage amongst orthopaedic surgeons that “grey hair equalds cuff tear” and the general teaching has been the cuff tears are a normal part of the ageing process. Sher et all in 1996 look at asymptomatic patients using magnetic resonance imaging. They found that 54% of the asymptomatic shoulders over the age of 60 years had evidence of irritated cuff tear, 28% of those were full thickness tears, and 26% were partial thickness tears. However, other studies comparing MRI scans with arthroscopic see were demonstrating that MRI scanning is only 75 -95% accurate in diagnosing rotator cuff tears. Therefore, the true incidence of degenerative tears of rotator cuff of asymptomatic shoulder is not exactly known
Is sub Acromial your decompression alone adequate for the treatment of rotator cuff tears?
Hoe-Hanson et al In 1999 looked at 39 patients undergoing sub cranial decompression alone. 13 partial tears and 13 patients with intact rotator cuff. On reviewing the patients at six years later they found that there was no significant difference between the groups with regarding to range of motion, strength and pain relief with no difference in the constant scores. They concluded that the functional outcome after arthroscopic sub Acromial Decompression was not obviously related to the post operative degree of cuff pathology, where there was a small rotator cuff tear
A similar study performed by Massoud et al (JBJS 2002) looked at sub acromial decompression alone for chronic small and medium sized cuff tears in 118 shoulders between two and five years after sub acromial decompression. They found a satisfactory outcome in 59% of patients under the age of 60 and 87.5% of those over the age of 60. An unsatisfactory outcome was related to manual work, duration of symptoms of more than twelve months and younger age. Further surgery in the form of a rotator cuff repair was required in 20% of the total number of patients in the study. They found that half of those tears had increased in size.
Ellman et al in Arthroscopy 1993 prospective study selected patients into three groups based on the size of tear measured during surgery, physiological aids, handedness and activity level. They found that small tears (less than 2cms) in older individuals not involved in strenuous activities did well with sub acromial decompression alone. Patients with larger tears (2-4cms) did poorly (50% satisfactory). With massive irreparable tears the pain relief was satisfactory on a limited goals basis but there was no improvement in strength or range of motion. Their study emphasised the importance of patient selection based on the above criteria in selecting the treatment for rotator cuff tears.
In other studies looking at sub acromial decompression alone and comparing it with rotator cuff repairs (Wiley 1991, Zyliac 1194, Godsman 1997, Savoie 1997) all found that with large rotator cuff tears there was deterioration over time and the results of the sub acromial decompression alone was inferior to rotator cuff repair.
In summary of the data thus far, it would appear that Arthroscopic Sub Acromial Decompression alone is good for pain relief in the presence of rotator cuff tears in elderly patients (>60 years) on a limited goals basis, patients with low functional demand and massive irreparable tears in elderly patients with low functional demand. Only one study (O’Hanson et al) demonstrated good results for sub acromial decompression alone for full thickness rotator cuff tears of a small size.
What is the natural history of Rotator Cuff Tears?
.
What are the results of rotator cuff repair?
The published results of rotator cuff repairs have been variable. This may be related to patient selection and older techniques.
Summary of few large studies:
|
Author, year |
No. |
F/up |
Tear size |
Exc/good |
|
Murray, Snyder 2002 |
48 |
Av 39 m |
Medium and Large |
96% |
|
Jones, FH Savoie 2003 |
50 |
1 – 5 yr |
Large and Massive |
88% |
|
Wolf 20 04 |
96 |
4 – 10 yr |
Full thickness |
94% |
|
La, Burkhart 2004 |
14 |
Av 23 m |
Large and Massive |
93% |
|
Author, year |
No. |
Mean Age (years) |
Average Follow-up (months) |
Excellent & good clinical results |
Cuff integrity (imaging method) |
|
Wolf et al, 2004 (20) |
96 |
57.6 |
78 |
94% |
Not done |
|
Bouileau et al, 2005 (16) |
65 |
60 |
29 |
92% |
71% (CTA) |
|
Charousset et al, 2008 (19) |
114 |
59.4 |
24 |
94% |
75% (CTA) |
|
*LaFosse et al, 2007 (18) |
105 |
52 |
23 |
94% |
89% (CTA) |
|
*Huijsmans et al, 2007 (21) |
264 |
59 |
22 |
91% |
92% |
[* indicates studies with double row rotator cuff repair technique only]
Most studies have only reported the size of the cuff tear and patient age in relation to the results. However, our understanding of the importance of the rotator cuff muscle quality (atrophy and fatty infiltration) in relation to repair results is now clearer.
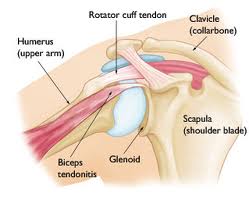
We also appreciate the relevance of the broad insertion area of the rotator cuff on thehumerus, known as the footprint area. We now attempt to recreate this with our repair techniques.
Progressive degenerative cuff tears are have poorer tendon quality than traumatic tears in good tendon tissue and are more likely to fail. Repair of these tears is likely to fail and we need to look at alternative methods to manage these patients, other than rotator cuff repair.
In summary, based on our understanding of the published literature and experience – Yes!
But… this does depend on a number of factors, not all of which are easy to objectively quantify. A traumatic rotator cuff tear in a young, active patient would be an indication for early repair. An atraumatic, degenerate tear in an elderly, low-demand patient would be not be a good candidate for repair. However, the grey zone between those two extremes is less clear and it is best to apply principles of shared decision making. I. Hence, decisions to proceed with rotator cuff repair are best supported with evidence based discussions regarding management options, complications, recovery times and anticipated outcomes.
PLEASE THIS IS FROM THE WEBSITE OF SHOULDER.CO.UK
Are you can see from this example of a Shoulder Examination there are other diagnosis such as SLAP tear
Members of BASEM are able to access excellent Education Videos Shoulder Examination Videos for good Clinical Practical


Shoulder exercises has been changed and Helen has attended a Shoulder Rehabilitation Course on by Jo Gibson this year held at Falkirk Courtesy of Stewart Kerr Physiotherapist Jo Gibson gave us all full 2 day conference on the
examination, diagnosis referral to shoulder surgeon or exercise prescription